Hearing and Down syndrome
Ask any parent of a young child with Down syndrome, and they would tell you that their biggest worry is speech. An important aspect of speech development is being able to hear well and clearly, and kids with Down syndrome are more likely to have hearing deficits than their typical peers.
Any unresolved hearing loss can further impede speech and language development, which is why the American Academy of Pediatrics and the Down Syndrome Medical Interest Group recommend hearing tests at birth and then every six months up to the age of three for kids with Down syndrome.
The ears of people with DS are a slightly different anatomically than typical people.
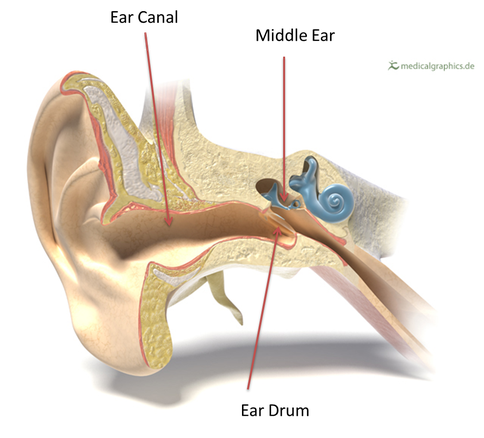
The Ear Canal, through which the sound travels into the ear, is narrower for people with DS and can get clogged up very easily with wax, muffling the sounds they hear.
The Middle Ear, for typical people slants downwards. A cold can cause mucus to fill in the middle ear and the downward slant allows for easy draining. For people with DS, the middle ear has very little slant, causing mucus to stick around and cause hearing loss.
These anatomical differences can cause Conductive Hearing Loss, which occurs in 60-70% of kids with Down syndrome (1).
Sensori-neural hearing loss is caused by issues in the inner ear, is pretty rare but does occur in some people with Down syndrome. This must be managed on a case-by-case basis by your child’s ENT specialist and audiologist and will not be discussed further in this article.
To monitor hearing for our kids, there are three types of hearing tests (2):
1. Auditory Brainstem Response (ABR)
This test examines the pathway that connects your ear to the part of the brain that processes the sound. During the test, your child will wear an earplug in each ear and electrodes on their head, which will measure their brain’s response as sounds are played through the earplugs.
This is the test performed at newborn screening and the one that provides the most information, but the child must stay absolutely still and preferably asleep for the results of the test to be valid. They can do this test on newborns easily and up to six months of age if the baby cooperates, but beyond that age, kids need to be sedated for this test.
2. Otoacoustic Emissions (OAEs) Test
This test measures the emissions given off by the inner ear when responding to a sound. This test measures hearing loss, but can also be indicative of blockage in the outer ear (wax) or middle ear (fluid).
An OAE test uses a probe placed in the ear canal for about 5 seconds. This is a very quick test, and is usually done every time your child goes in for a hearing test.
3. Pure-tone testing
This is a behavioral test that requires the child’s active participation, and is most used for kids over the age of 1. This test helps find the quietest sound they can hear at different pitches, or frequencies. The child is asked to wear earphones and respond when they hear the sound.
For younger children, the audiologist will teach the child to look where the sound came from and a light or toy will be seen near the speaker, and slightly older kids might be asked to do some action in a game every time they hear a sound. Over time, kids learn to cooperate better for this test, but sedated ABRs maybe needed till then if hearing loss is suspected.
4. Bone Conduction Testing
Audiologists use a type of hearing aid in this test when they suspect that something, such as wax or fluid, is blocking the outer or middle ear. The sounds sent through this device cause the skull to gently vibrate. This vibration goes to the inner ear, or cochlea, and skips any wax/fluid issues in the outer or middle ear.
For this test, the audiologist will put a small device on a headband behind the ear or on the forehead and do the pure-tone testing.
Your child might “fail” a hearing test even you think they are hearing perfectly fine based on your observation of your child at home. The picture below is an audiogram (3) which shows how much a child hears at various levels of hearing loss.

A child with “Normal” hearing hears sounds of every pitch at a soft level. A child with “Mild” hearing loss hears most speech sounds from a close distance. A child with “Moderate” hearing loss may hear vowel sounds (louder sounds) in speech. What we perceive as hearing loss as non-experts, not responding to calls and louds sounds, is considered severe or profound hearing loss by experts.
Most conductive hearing loss due to fluid/wax falls in the mild-moderate hearing loss range, which means our children might be able to hear and respond to us in 1:1 conversations, but have trouble hearing certain consonants and lower pitch voices like that of their fathers. If they cannot hear certain consonants, they cannot reproduce them in speech, and hence, we must treat conductive hearing loss and give them every advantage of hearing clearly.
Treating Conductive Hearing Loss
Wax in the outer ear
If the audiologist/ENT sees a lot of wax in the outer ear, you might be asked to use wax removal drops to loosen and remove the wax, and return for a follow-up test. Some ENTs will also use a suction device to clean out the wax during the office visit.
It is a good practice to do wax-removal ear-drops on our kiddos every week, given how easily their narrow ear canals can be blocked up with wax and compromise their hearing. Your pediatrician can recommend or prescribe them during a regular visit.
Fluid in the middle ear
If the outer ear looks clear and test results are still indicating hearing loss, it is likely there is fluid in the middle ear.
The fluid is usually treated with PE tubes, surgically placed in the eardrum, to allow the fluid in the middle ear to drain outward to the outer ear. Having this done for your infant can be nerve-wracking, but rest assured that it is a routine and very minor surgery.
The tubes fall out as kids grow and you might need new set of tubes annually. The fluid draining action of the tubes also helps reduce occurrence and severity of ear infections along with preserving hearing, so that is a nice bonus.
Tubes can get blocked by outer ear wax too, so it is important to continue weekly wax removal drops to keep them clear. Peroxide-based ear drops (like Debrox) might cause pain and tingling when they go through the tube into the middle ear, so kids with tubes might need to use oil-based ear drops.

Solution for persistent conductive hearing loss
If the fluid and wax issues are persistent, hearing loss returns within a few months of tubes being placed, and new tubes are needed too often, bone-conduction hearing aids might be a good idea to consider. These are non-invasive hearing aids, with a small device on a headband that makes the skull vibrate gently, vibrations that travel from the skull to the inner ear to enable hearing.
The hearing aid companies provide loaner devices for a 3-month free trial, and your child’s audiologist can organize the loan, and provide a tutorial and fitting.
Headphones and sunglasses with bone-conduction technology are available for use for the general population too. They allow you to hear music without blocking your ears to ambient sounds and are pretty popular among runners and bikers.
It is natural to worry about surgery to place ear tubes, about our child’s cooperation and trauma around testing, and about hearing aids making our child look different from their peers. Even though these worries and fears are valid, we need to overcome them, and do what needs to be done to maintain our child’s hearing. Most kids eventually grow out of conductive hearing loss as the size of their ears grows with age, but maintaining their ability to hear well in the early years of language acquisition and speech development is pivotal to our kids’ development.
To read more from Sruthi Muralidharan or to follow her blog, No BS About DS, click the link below.